March 27, 2020
Primary repair remains the treatment of choice for primary patellar and quadriceps tendon rupture. However, extensor mechanism rupture is a more challenging problem in the setting of tendinopathy or previous surgery or in conjunction with a knee dislocation.
Aumento del injerto de cuatro hebras
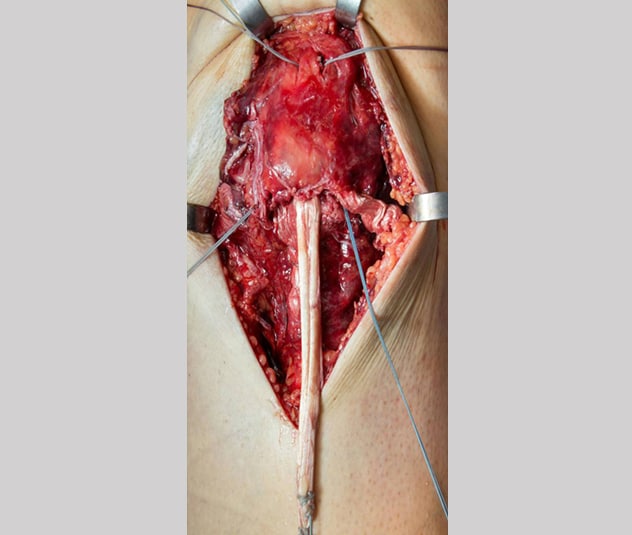
Aumento del injerto de cuatro hebras
La fotografía intraoperatoria muestra el autoinjerto semitendinoso doblado en el hueco de la rótula distal, las suturas transóseas atadas sobre el polo rotuliano proximal y los anclajes de sutura en el polo rotuliano distal. La longitud del tendón semitendinoso permite un aumento del injerto de cuatro hebras.
Mayo Clinic uses a novel tendon augmentation technique for select patients with these injuries. Described in the May 2016 issue of the Journal of Knee Surgery, the procedure consists of a primary patellar or quadriceps tendon repair with semitendinosus autograft augmentation using a proximal or distal patellar socket. Although Mayo Clinic's original technique preserved the semitendinosus tendon insertion, the current preference is to use a free four-stranded graft. The benefits include the addition of autogeneic tissue, decreased risk of patellar fracture from transverse or longitudinal bone tunnels, fewer hardware complications, and accelerated rehabilitation.
"It comes down to the fact that normal tendons don't tear," says Michael J. Stuart, M.D., an orthopedic surgeon at Mayo Clinic in Rochester, Minnesota. "A tendon with a predisposition to rupture doesn't have the same healing potential after surgical repair as a normal tendon. Augmentation with a semitendinosus autograft can provide a high-strength construct with distinct advantages."
Patellar or quadriceps tendon repair and augmentation might be performed for select patients with chronic tendinopathy and poor tissue quality as well as patients with prior tendon debridement or failed primary tendon repair.
"The goal is to improve the patient's rate of healing with reliable return of extensor mechanism strength and preinjury activity levels," Dr. Stuart says. "This technique also allows for an accelerated rehabilitation program. Traditionally, if the strength of the repair was a bit tenuous, we would have to immobilize the knee for an extended time with delayed joint motion and strength training. We are confident that the strength of the augmented construct promotes immediate range of motion and progressive resistance strength training with better results and earlier return to work, sports and activities."
Dr. Stuart cites the case of a 22-year-old professional football player who had undergone right knee patellar tendon debridement for chronic tendinopathy but experienced persistent anterior knee pain with all activities. He achieved full active range of motion six weeks after patellar tendon repair with semitendinosus autograft augmentation surgery at Mayo Clinic. Six months after surgery, the patient resumed all activities without restrictions. Two years after surgery, the patient had retired from football but experienced full knee range of motion and no pain.
"It's pretty impressive how quickly patients regain knee motion," Dr. Stuart says. "We have not experienced reoperations, repair failures, hardware complications or patellar fractures to date. The outcomes have been great."
For more information
O'Malley M, et al. Extensor mechanism disruption in knee dislocation.1055/s-0035-1568991 Journal of Knee Surgery. 2016;29:293.