Oct. 18, 2023
Congenital ear differences are complex, and they can affect the external and middle ear, physical appearance, and ability to hear. Likewise, ear reconstruction to restore form, hearing function and a natural appearance of the ear also is a complex process.
A multidisciplinary team of specialists at Mayo Clinic Children's Center focuses on caring for children with ear differences. Pediatric Plastic and Reconstructive Surgery, Audiology, Otolaryngology (ENT), and Cleft and Craniofacial Clinic specialists work together on comprehensive treatment plans to ensure quality care, successful recovery and best outcomes.
Pediatric ear irregularities can include:
- Microtia — an underdeveloped ear.
- Anotia — a missing ear.
- Cryptotia — a part of the ear is buried under the skin on the side of the head.
- Stahl's ear — a pointed ear that has extra folds of skin.
- Constricted ear — an ear that is folded over itself.
- Damaged ear — such as from cancer treatment, trauma or burns.
"While ear reconstruction primarily focuses on the outer part of the ear," says Waleed Gibreel, M.B.B.S., a plastic surgeon at Mayo Clinic in Rochester, Minnesota, "treatment of hearing issues are also prioritized."
Early referral, testing and evaluation is a common theme for successful intervention in pediatric patients of all ages. "A hearing assessment and overall evaluation is vital in the early stages," says Samir Mardini, M.D., a plastic surgeon at Mayo Clinic in Rochester, Minnesota. "Early evaluation ensures a comprehensive plan can be established to cover their coexisting diagnoses. If not, a child might undergo a surgery that makes some of the treatment options nonviable."
 小儿外科重建术
小儿外科重建术
这种手术方法使用一种医用植入物(称为多孔聚乙烯植入物)作为耳支架。
There are several approaches to ear reconstruction, depending on patient's age and severity of the malformation:
-
Ear molding. Molding is a noninvasive approach but requires early intervention. "We've seen newborns that have all the structures of the ear, but the outward appearance is malformed and lacks the normal folds and curves," says Dr. Gibreel. "These babies can benefit from ear molding, but to be effective it must take place when the child is between 7 and 10 days old, when estrogen levels are still high in their blood and the cartilage is still pliable.
"If a pediatrician is unsure whether a patient is good candidate for early molding, we recommend referral when the child is 1 to 2 weeks old for evaluation, as it's a time-sensitive intervention," says Dr. Gibreel.
-
Reconstruction with rib cartilage. Autologous reconstruction is often used for children who are missing most or all parts of the external ear structures, such as microtia or anotia. In those cases, surgery is usually performed between ages 8 and 10 years old, when there's enough rib cartilage available for the procedure.
This approach typically involves 3 to 4 surgeries, depending on the preferred technique. The order of the surgeries varies depending on the technique. The surgeries include:
- Harvesting cartilage from the ribs and carving the framework that looks like an ear.
- Positioning the framework under the skin at the ear site.
- Creating a tragus and ear lobule.
- Elevating the ear away from the head.
"One of the advantages to this approach is using the child's own cartilage, as opposed to foreign material, which has its own risks," says Dr. Gibreel. "Of course, by addressing one difference in the body by creating a difference in another area can be a concern. The inclusion of our pediatric psychiatrists throughout the process is an essential part of our whole-person care approach."
-
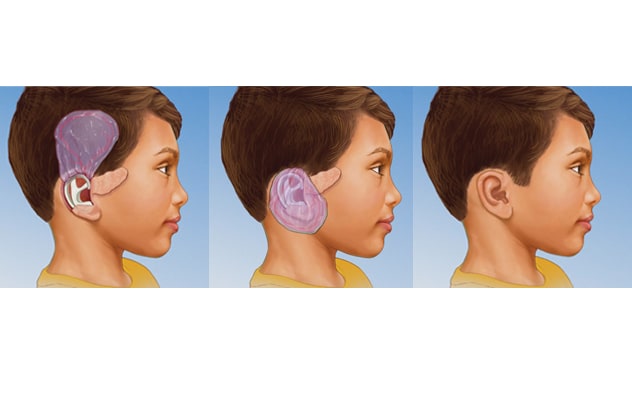
Reconstruction with a flap and an implant (porous polyethylene implant). Instead of using cartilage from the ribs, this surgical approach uses a medical implant for the ear framework. The surgeon places the implant at the ear site and covers it with a flap. This is a thin membrane of tissue underneath the scalp called temporoparietal fascia. The flap is then covered with a skin graft. Typically, reconstruction using an implant requires only one surgery. Children as young as 3 or 4 years old may be able to have this surgery, as the ear reaches 85% of its adult size around that age, and it reaches its adult size around 5 to 6 years of age. This reconstructive technique gives children the opportunity to have a fully reconstructed outer ear before they go to school. This enhances their ability to integrate with other kids without feeling different during the early years of childhood.
Mayo Clinic offers innovative, custom porous polyethylene implants designed to precisely match the patient's nonaffected ear. In patients who are missing only one ear, "A laser scan of the patient's normal ear is taken and serves as a model for a 3D-printed porous polyethylene implant," says Dr. Gibreel. "Only a few healthcare centers in the world have access to this technology, and we're pleased to be able to offer this option to our patients. This is just one way we strive to ensure each patient has the best outcome, in terms of function and natural appearance."
- Placement of a prosthesis. With this type of ear reconstruction, a prosthesis is surgically anchored into the bone at the ear site. This approach may be used when ear tissue is severely damaged, as with a burn. It also may be used when a large part of the ear is missing due to cancer surgery or when another ear reconstruction approach failed. Prostheses are typically used in adults rather than children.
"With a comprehensive evaluation and individualized treatment plan in place," says Dr. Mardini, "our specialists coordinate comprehensive care at Mayo Clinic Children's Center, and they also collaborate closely with a patient's local physician for follow-up care at home, to help ensure a smooth transition and continued recovery."
For more information
Refer a patient to Mayo Clinic.