April 10, 2024
Best treatment methods have been controversial in instances in which physicians discover endometriosis in the bowel, a location far outside the uterine lining where endometrial cells are commonly expected, according to Carrie L. Langstraat, M.D., a gynecologic oncologist at Mayo Clinic in Minnesota. Potential treatments have included observation, ablation, medical management and surgical excision of all endometrioses present in the bowel.
When endometriosis is found in the bowel, surgical excision is advisable, says Dr. Langstraat. According to an article she and her colleagues published in the September 2022 issue of Journal of Minimally Invasive Gynecology, GYN surgeons must consider an array of techniques in this situation:
 蘑菇帽状病变
蘑菇帽状病变
蘑菇帽状病变需要进行分段切除术
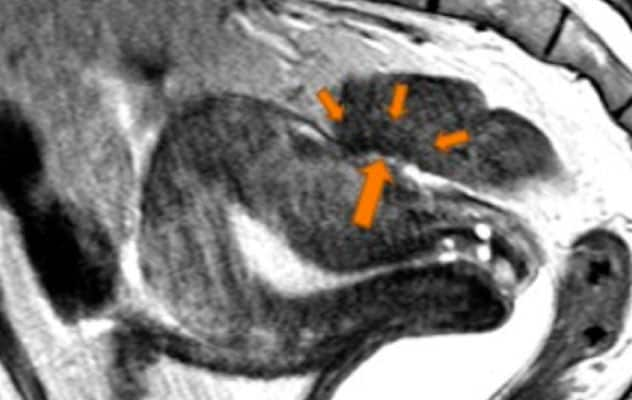 深层侵入性肠道病变
深层侵入性肠道病变
需要进行盘状切除的深层侵入性肠道病变。
- Complete resection. This involves manual resection with primary suture closure or use of a regular stapler transabdominally or an end-to-end anastomosis stapler transrectally. If the lesion is greater than 3 cm and involves more than half of the bowel's circumference, or if multifocal lesions are present, the surgeon performs a segmental resection.
- Discoid resection. This is appropriate for lesions of less than 1 to 2 cm that involve the muscularis and less than one-third to one-half of the bowel's circumference.
- Serosal shaving. This approach is appropriate for lesions with little muscularis involvement. It can be done sharply or with electrosurgery. The surgeon must order bowel function evaluation after the shaving procedure.
Patients with bowel endometriosis may experience pain, bloody stool or infertility, the last of which may arise as the sole bowel endometriosis symptom. For patients who have complete resection, Dr. Langstraat confirms anecdotally that infertility and pain improve and recurrent endometriosis rates in the bowel decrease.
Zaraq Khan, M.B.B.S., a fertility specialist and a minimally invasive GYN surgeon with expertise in advanced endometriosis at Mayo Clinic in Minnesota, discovered during his fellowship training that patients presenting with infertility would at times have advanced endometriosis. Yet he did not observe interdisciplinary work spanning these two conditions.
"This was a disconnect," says Dr. Khan. "I wanted to be a bridge between fertility and advanced surgical approaches to endometriosis. GYN surgery at that time did not specialize in fertility-sparing endometriosis surgery, so I wanted to learn how to do that."
He explains that historically, when excising endometriosis, GYN surgeons removed not only the endometriosis but also the ovaries and uterus to provide more definitive care to patients.
Today, when endometriosis is hindering a patient's fertility, a surgeon sometimes recommends preconception removal of only the tissue affected by disease, with ovarian- and uterine-sparing techniques, indicates Dr. Khan. Once the patient becomes pregnant and delivers, the surgeon removes additional disease without uterine sparing if there is a recurrence.
The nature of bowel endometriosis
The etiology of endometriosis in general, including bowel endometriosis, remains elusive, according to Dr. Khan. Endometriosis commonly occurs in the ovaries, fallopian tubes and uterus and surrounding areas referred to as pelvic peritoneum.
The average time from the onset of a patient's endometriosis to diagnosis averages about six years, says Dr. Khan.
"Many patients spend years being told by physicians there's no detectable problem, and yet they are in pain and can't have a baby," he says.
Intrinsic to bowel endometriosis is that "if you're not looking for it, you're not going to find it," says Dr. Langstraat. It appears in different phenotypes and distributions.
Dr. Khan says he never saw bowel endometriosis in his training due to lack of an imaging protocol for locating this type of endometriosis. He explains that physicians often find bowel endometriosis when ordering imaging for another purpose.
Detection issues abound with bowel endometriosis, according to Drs. Khan and Langstraat. Even when performing an MRI, radiologists not looking for bowel endometriosis typically do not see it or find it. At other times, radiologists observe bowel endometriosis but the gynecologist is not comfortable with surgical removal. Beyond actively looking for bowel endometriosis, Dr. Langstraat recommends a biopsy for pathological confirmation.
Dr. Khan calls for collaboration among physicians specializing in gastroenterology, urology, radiology, gynecology and fertility to address bowel endometriosis.
"We see bowel endometriosis all the time, yet people don't understand this disease," he says.
Bowel endometriosis treatment
Dr. Langstraat indicates that leaking or infection risks from surgical removal of bowel endometriosis are considerable.
"You need specific training to prevent and manage complications related to bowel endometriosis resection," says Dr. Langstraat.
Due to these risks, bowel endometriosis treatment follows symptoms, according to Dr. Khan. In other words, if a radiologist discovers endometriosis yet the patient is asymptomatic, endometriosis specialists may elect to observe the condition over time.
Though discoid resection of endometriosis of less than 1.5 cm may be easily debulked and removed with stapling, Dr. Langstraat says that serosal shaving is not a surgery to perform without adequate training and the assistance of a colorectal surgeon. Segmental resection can prompt long-term side effects, she says, such as alternating diarrhea and constipation. These side effects likely are due to the lesion's size, she indicates. Dr. Langstraat hopes future research will better illuminate the origins and means of addressing these side effects.
Dr. Khan notes that knowledge of bowel endometriosis excision is rare outside of those specializing in endometriosis surgery.
"Bowel endometriosis is difficult to excise, and it's not to be tackled by those who are unfamiliar," says Dr. Khan. "You need an endometriosis excision specialist, often with a multidisciplinary surgical team."
Obstetrics and Gynecology at Mayo Clinic in Minnesota has such specialists and welcomes referrals for bowel endometriosis excision.
For more information
Warring SK, et al. Excision of deep endometriosis of the rectosigmoid: individualizing care to the presenting pathology. Journal of Minimally Invasive Gynecology. 29;2022:1037.
Refer a patient to Mayo Clinic.