Diagnosis
Meningioma
Meningioma
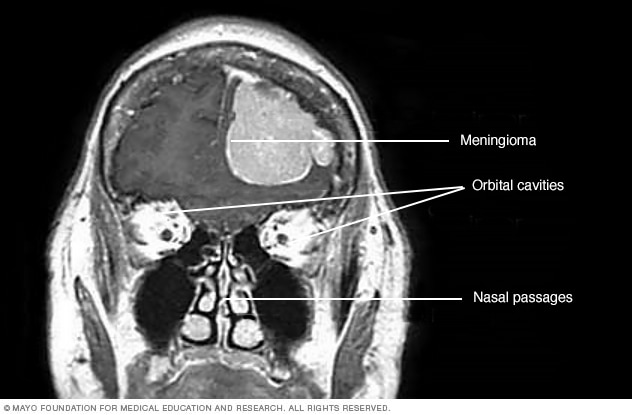
This contrast-enhanced MRI scan of a person's head shows a meningioma. This meningioma has grown large enough to push down into the brain tissue.
A meningioma can be hard to diagnose because the tumor is often slow growing. Symptoms may be subtle and thought to be other health conditions or signs of aging. Many meningiomas are found by chance during brain imaging done for other reasons.
If your healthcare professional suspects a meningioma, you may be referred to a doctor who specializes in conditions of the brain and spine, called a neurologist.
Diagnosis usually starts with a review of your medical history and symptoms, followed by a physical and neurological exam. The doctor checks your vision, hearing, balance, coordination, strength and reflexes. If the exam suggests a concern, your care team orders imaging with contrast.
Imaging tests with contrast may include:
- Brain MRI. This test uses magnetic fields and radio waves to make detailed pictures of the brain. It's the preferred imaging test for seeing a meningioma and how it affects nearby tissue.
- Brain CT. This test uses X-rays to create cross-sectional images of the brain. An iodine-based contrast may be used to highlight certain areas, and CT is especially helpful for showing bone changes.
Sometimes, a biopsy is done to confirm the tumor type and grade. A biopsy isn't always needed because MRI findings can be enough to suggest a meningioma. When needed, a biopsy provides tissue for study under a microscope to confirm the diagnosis and grade.
Tumor histology and WHO grade
Histology means how the tumor cells look under a microscope. A biopsy allows the lab to study these cells and assign a grade based on the World Health Organization (WHO) classification system. Grade 1 cells look more organized and usually grow slowly. Grades 2 and 3 have more active or irregular cells that are more likely to come back after treatment.
Imaging can suggest a meningioma, but only a biopsy — looking at tumor cells under a microscope — can confirm the tumor type and grade. The pathology report helps predict how fast the tumor may grow and guides the care plan.
What this means for you: Histology and grade help the care team choose next steps. Many grade 1 tumors can be managed with surgery or observation. Grade 2 and 3 tumors are more likely to need added treatment, such as radiation, to lower the chance of the tumor returning. In some cases targeted therapies and clinical trials are an option.
More Information
Treatment
The goals of meningioma treatment are to control manage the tumor, protect neurological function and maintain quality of life. Decisions are based on what the tumor looks like on scans, the WHO grade from the lab, and your health and personal preferences. A team that may include specialists in neurology, neurosurgery, radiation oncology, neuroradiology and neuropathology works together to guide your care.
Meningiomas don't all need the same approach. Some can be safely watched, some are best treated with surgery first, and some benefit from radiation either instead of surgery or after it. Your care team reviews your MRI and biopsy results, talks through benefits and risks, and helps you choose the plan that fits your goals.
Meningioma treatment depends on several factors:
- Tumor size and location.
- Growth rate.
- Age and overall health.
- Personal goals for care.
These details help your care team decide whether the best approach is observation, surgery, radiation or a combination.
Wait-and-see approach
Not everyone needs treatment right away. A small, slow-growing meningioma that isn't causing symptoms may not need intervention.
This approach, known as observation or active surveillance, involves regular imaging and follow-up visits to watch for changes in the tumor or symptoms. If scans later show the tumor is growing or causing symptoms, your care team may recommend surgery or radiation.
Meningioma surgery and recovery
When the tumor causes symptoms or grows, surgery is often the first step. Surgeons remove as much tumor as safely possible.
After surgery:
- If no tumor remains, follow-up scans are usually all that's needed.
- If a small benign portion remains, observation or targeted radiation may follow.
- If the tumor is irregular or cancerous, radiation is often added and targeted therapies along with clinical trials may be considered.
Surgery risks include bleeding or infection. Procedures near the optic nerve may affect vision.
Surgical approaches
Because meningiomas can grow in many parts of the brain and skull, surgeons use different approaches to reach and safely remove them. The goal is always to take out as much of the tumor as possible while protecting healthy tissue. Your team may use:
- Craniotomy, where a small part of the skull is opened to reach the tumor.
- Keyhole craniotomy, using a smaller opening for quicker recovery.
- Endoscopic endonasal surgery, entering through the nose to reach certain skull base tumors.
Each technique has benefits and risks depending on the tumor's size and closeness to vital nerves or blood vessels.
Meningioma surgical treatment by location
| Tumor location |
Treatment and outlook |
|
Frontal lobe
|
Usually easier to reach. Full removal often leads to good recovery and low chance of coming back.
|
|
Bone near the eye, called the sphenoid wing
|
May need surgery plus focused radiation if full removal could affect vision. Treatment often controls growth while protecting vision.
|
|
Deep skull area near the brainstem, called the petroclival region
|
Complete removal may not be safe. Partial removal can lower the risk of nerve or brainstem injury and often controls growth.
|
|
Midline of the brain, called the parasagittal or falx
|
Surgeons remove as much as is safe while protecting blood flow. Careful surgery often leads to long-term control of tumor growth.
|
|
Outer surface of the brain, called the convexity
|
Often easy to reach. Surgery can usually remove the tumor completely, which often leads to good long-term control of tumor growth.
|
|
Spine or spinal cord
|
Often easy to reach. Surgery can often remove the tumor completely, leading to good long-term control of tumor growth.
|
|
Large veins in the brain, called the venous sinuses
|
Complete removal may not be safe. Partial removal plus radiation can control tumor growth.
|
Recovery from meningioma surgery is different for everyone. Healing can take weeks to months depending on size and location. Early movement, physical therapy and follow-up visits aid recovery.
Radiation treatment for meningioma
Radiation may follow surgery or serve as primary therapy when the tumor can't be safely removed. It destroys remaining cells, lowers recurrence risk, and can improve long-term survival.
Types of radiation used to treat meningioma may include:
- Brain stereotactic radiosurgery (SRS). This radiation treatment delivers strong, focused radiation directly to the tumor. It's usually done in one session, so most people can go home the same day.
- Fractionated stereotactic radiotherapy (SRT). This treatment delivers small doses of radiation over several sessions. It's often used for larger tumors or those near sensitive areas, such as the optic nerve.
- Intensity-modulated radiation therapy (IMRT). This approach shapes and adjusts the radiation beams to match the tumor's outline, helping protect nearby healthy tissue.
- Proton beam therapy. This method uses positively charged particles called protons to destroy tumor cells while reducing radiation exposure to surrounding tissue.
Medicines and targeted therapy
Medicines are sometimes used after surgery and radiation if any tumor cells remain or the tumor grows back. They're also considered when surgery or radiation isn't possible. Most meningiomas don't respond well to standard chemotherapy, so drug treatment is usually part of a clinical trial. Researchers are studying targeted drugs that act on tumor growth signals.
These are some of the medicines studied so far for meningioma:
- Bevacizumab can reduce swelling and may slow tumor growth in some people, but results differ and more research is needed.
- Bevacizumab plus everolimus has helped some tumors stay the same size in small studies, but it has not been shown to help people live longer.
- Somatostatin-pathway drugs, such as octreotide, may keep the tumor from growing in some people, but the evidence is limited.
- Tyrosine kinase inhibitors, such as sunitinib, have shown mixed results across small studies and are still considered experimental.
- Immunotherapy, such as pembrolizumab, has been tried for high-grade tumors that come back, but early results are limited. It's best pursued in a clinical trial.
What this means for you: If the tumor grows after surgery and radiation, your care team may discuss clinical trials for targeted drugs or immunotherapy that match the tumor's biology.
Typical meningioma treatment paths
| Tumor grade |
Typical treatment approach |
| Grade 1 |
Observation, surgery if needed, then follow-up imaging |
| Grade 2 |
Surgery, radiation, then regular MRI follow-up
|
| Grade 3 |
Surgery, radiation, then ongoing monitoring or clinical trials
|
More Information
More Information
Clinical trials
Explore Mayo Clinic studies testing new treatments, interventions and tests as a means to prevent, detect, treat or manage this condition.
Alternative medicine
Alternative and complementary therapies don't treat meningioma tumors. But they can help with stress, sleep, pain, nausea and mood during or after treatment. They should be used alongside your medical care, not instead of it.
How it helps
There are many types of alternative medicine. Here's how each type may help:
- Acupuncture. Can ease nausea, hot flashes or some types of pain.
- Massage therapy. May reduce muscle tension and anxiety.
- Meditation and relaxation exercises. Can lower stress and improve sleep.
- Music therapy. May improve mood and help with coping.
- Hypnosis. Sometimes used for anxiety, nausea or procedure-related stress.
Safety first
Tell your care team about any therapy you plan to try so they can check for safety with surgery, radiation or medicines. Avoid deep tissue massage over radiation areas or recent surgery sites.
Skip herbs or supplements unless your care team approves. Some can interact with medicines or affect bleeding risk.
When to avoid supportive therapies
If you have headaches that can't be controlled, new vision changes, new weakness or new seizures, seek medical care first.
Delay acupuncture or massage if you have low platelets, active infection or open wounds.
How to choose a practitioner
Look for licensed professionals who have experience with people who have brain or spine tumors. Ask them about their training, infection control, and how they coordinate with your care team.
What this means for you: Supportive care can make treatment more comfortable and daily life easier. Use these options to help manage side effects and stress. Check in with your care team to choose what's safe and helpful for you.
Coping and support
A meningioma diagnosis can disrupt your life. You have visits to doctors and surgeons as you prepare for your treatment. To help you cope, try to:
-
Learn all you can about meningiomas. Ask your healthcare team where you can learn more about meningiomas and your treatment options. Visit your local library and ask a librarian to help you find good sources of information, including online sources.
Write down questions to ask at your next appointment with your healthcare professional. The more you know about your condition, the better able you'll be to decide about your treatment.
-
Build a support network. It can help to have someone to talk with about your feelings. Other people who can support you include social workers and psychologists. Ask your healthcare professional to refer you. Talk with your pastor, rabbi or other spiritual leader.
It also can help to talk with other people with meningiomas. Think about joining a support group, either in person or online. Ask your healthcare team about brain tumor or meningioma support groups in your area. Or contact the American Brain Tumor Association.
-
Take care of yourself. Eat a diet rich in fruits and vegetables. Get moderate exercise daily if your healthcare professional OKs it. Get enough sleep to feel rested.
Reduce stress in your life. Focus on what matters to you. These measures won't cure your meningioma. But they may help you feel better as you recover from surgery or help you cope during radiation therapy.
Preparing for your appointment
You can start by seeing your main healthcare professional. From there, you may be referred to specialists who treat brain conditions, such as neurologists and neurosurgeons.
Here's some information to help you prepare for your appointment.
What you can do
- Be aware of any pre-appointment restrictions. When you make the appointment, be sure to ask if there's anything you need to do in advance, such as restrict your diet.
- Write down any symptoms you have, including any that may seem unrelated to the reason for which you scheduled the appointment and when they began.
- Write down key personal information, including any major stresses or recent life changes.
- Make a list of all medicines, vitamins or supplements you take, including doses.
- Take a family member or friend along, if possible. Someone who goes with you can help you remember the information you get.
- Write down questions to ask your healthcare professional.
Preparing a list of questions will help you make the most of your time. For a meningioma, some basic questions to ask include:
- Is my meningioma cancerous?
- How large is my meningioma?
- Is my meningioma growing? How quickly?
- What treatments do you suggest?
- Do I need treatment now? Or is it better to wait and see?
- What are the potential complications of each treatment?
- Are there long-term complications I should know about?
- Should I seek a second opinion? Can you suggest a specialist or hospital that has experience in treating meningiomas?
- Are there any brochures or other printed material that I can have? What websites do you suggest?
- Do I need to decide about treatment right away? How long can I wait?
Be sure to ask all the questions you have.